DIALYSIS ACCESS
What is dialysis access
Kidneys work by constantly filtering the blood which removes excess water and nitrogen waste. They also work to regulate the electrolytes in the body. When the kidneys fail, these functions no longer work. This leads to a buildup of waste, excess fluid, and imbalances in electrolytes. It can cause death within a matter of days. Dialysis access surgery allows the blood to be accessed and treated. In order to filter the blood, vascular surgeons create either an arteriovenous fistula (AV fistula) or graft. An AV fistula is a direct connection between a vein and an artery. A graft is a tube connected at one end to an artery and at the other end to a vein.
Dialysis is a process where blood from a patient’s body is filtered by removing the waste products, balancing the electrolytes, and removing excess fluid. The dialysis machine exists outside the patient’s body. Blood has is removed from the body, sent through the machine to be filtered, and then returned back to the body. This is usually done 2-4 times per week and lasts about 3-4 hours a session. With dialysis, patients can live for many years despite having kidneys which no longer function.
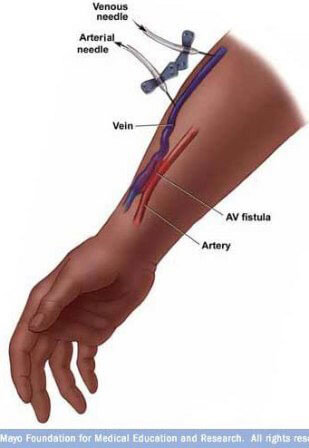
A dialysis access fistula creates a connection between a large artery and a large vein. Blood flow through the graft or fistula increases tremendously because of the pressure differences between an artery and the vein. This increased blood flow allows dialysis to occur by placing two large needles into the graft or fistula. The first needle pulls the blood out of the body, sending it to the dialyzer for filtration. The second needle returns the filtered blood to the body. The increased flow in the fistula is what allows this filtration to occur at a pace that filters all the blood in just a few hours. This would be impossible in an ordinary small vein or small artery.
Dr Aquino works closely with nephrologists and their patients to coordinate dialysis access.
Choosing to receive dialysis
The choice to receive dialysis is a difficult one. It is a choice that is best addressed along with the counseling a primary care doctor and nephrologist (kidney doctor). A dialysis access (AV fistula or AV graft) should be considered several weeks before it is time to begin dialysis. A nephrologist refers a patient to a vein specialist to create a dialysis fistula.
Planning for a fistula or graft
The vein doctor discusses different options. Determination of whether to place a graft or a fistula depends on the quality and size of the veins in the arm. Vascular surgeons typically prefer fistulas over grafts because they have a lower chance of becoming infected and they typically last much longer. However, a graft may be preferable if the veins are not large enough to create a fistula or if dialysis is imminent. Grafts are usable after a few weeks whereas fistulas take several weeks to mature (for the vein to get larger) prior to use.
The vein surgeon consideres several factors to determine what kind of surgery to perform. Planning is critical because fistulas and grafts do not last forever. Chances are the patient will need multiple subsequent access procedures over time. Surgeons usually place the first fistula or graft in the non-dominant arm. If the patient is right handed, the surgeon places the fistula in the left arm. The surgeon usually places it as low as possible in the forearm.
An ultrasound typically helps to decide which surgery is best. The ultrasound shows the surgeon the quality and size of the veins in both arms and allows her to plan the best procedure. Sometimes surgeons use the ultrasound to evaluate the quality of the arteries in the arm as well.
The patient also has a very important role in the weeks leading to dialysis. In order to have a successful dialysis access, the arm veins and arteries must be in good condition. It is critical that the patient protect his or her dialysis arm, both before and after the dialysis access surgery. This means avoiding blood draws in this arm at all times. A doctor or nurse can take blood pressure in the arm that doesn’t have the dialysis graft. It is important not to sleep with this arm underneath the head or neck because this can cut off the circulation. It is also important to avoid wearing tight clothing or jewelry on this arm, and to avoid using the arm excessively.
Dialysis access surgery
Dialysis access surgery typically happens on an outpatient basis. After the surgery, the patient will feel a “thrill” over the graft or fistula. A “thrill” is the increased flow of blood that occurs when blood goes from a high pressure arterial system to a low pressure venous system. It shows the fistula or graft is functioning correctly. The patient should feel for the “thrill” every day and contact their vascular surgeon immediately if they cannot feel it. This could mean the fistula or graft is no longer functioning. Usually dialysis grafts are used a few weeks after the procedure and a dialysis fistula can be used about 8-12 weeks after the procedure.
Dialysis graft
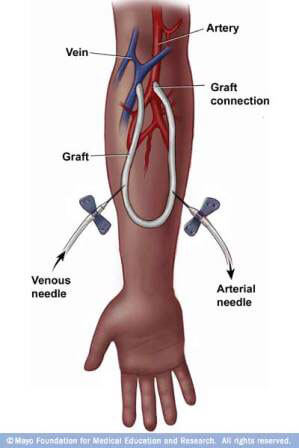
 Dialysis access surgery typically consists of one or two small incisions. In the case of a graft, a gortex tube is connected at one end to a vein and at another end to the artery. The surgeon plants the graft just under the skin which allows nurses to place needles easily into the length of the graft for dialysis.
Dialysis access surgery typically consists of one or two small incisions. In the case of a graft, a gortex tube is connected at one end to a vein and at another end to the artery. The surgeon plants the graft just under the skin which allows nurses to place needles easily into the length of the graft for dialysis.
Dialysis fistula
In the case of a fistula, the surgeon makes an incision over the artery and vein. The surgeon harvests the vein and divides it. One end of the vein is attached to the side of the artery. Dialysis staff will place the needles for dialysis in the vein itself. They will pull blood out and put blood back into the body. After surgery, the vein will grow slowly over several weeks. until it is prominent under the skin and big enough to get the needle in every time.
Maintaining dialysis access
The dialysis center tests the flow through a dialysis fistula or graft to ensure it’s functioning well. If a graft or fistula shows signs of decreasing flow, or increasing pressure, the patient goes back to the vascular surgeon for evaluation as sometimes a narrowing can occur in the graft or fistula.
At The San Francisco Vein Center, we are very invested in making sure our dialysis access lasts as long as possible. Dialysis patients usually become like members of our own family, and we take care of them accordingly! After surgery, regular ultrasounds help the surgeon evaluate the fistula regularly. If there is a narrowing or any other problem in our graft or fistula, we can act quickly to fix it before the access fails.
Treating failing fistulas or grafts
 If testing reveals problems in the fistula or graft, the surgeon makes every effort to correct the problem and keep the access working. Usually problems with flow are because of a narrowing within the vein portion of the fistula or graft. The surgeon treats this narrowing with angioplasty and/or a stent.
If testing reveals problems in the fistula or graft, the surgeon makes every effort to correct the problem and keep the access working. Usually problems with flow are because of a narrowing within the vein portion of the fistula or graft. The surgeon treats this narrowing with angioplasty and/or a stent.
In this procedure, the patient goes to the hospital for a fistulogram. For a fistulogram, the surgeon injects a small amount of dye into the fistula and takes pictures. This shows the narrowing in the vein. The surgeon then places a balloon at the exact location of the narrowing and inflates it before removing the balloon. Surgeons may also use stents to correct this narrowing problem. A stent is a small metal tube the surgeon deploys at the location of the vein stenosis. It holds the vessel open.
After the procedure, the patient usually goes home the same day and their dialysis regimen continues on the same schedule.
If a graft fails and clots, the patient goes directly to the hospital for evaluation and treatment. The surgeon decides if the clot must be removed from the graft or if a new graft or fistula is needed. Ultrasounds and fistulograms are employed when appropriate. If a new access is necessary, this is done in the operating room, much like the initial procedure. Because dialysis is done every two days, an adequate access must always exist for dialysis. If there is any question regarding the use of a graft or fistula, a dialysis catheter will be inserted.
Dialysis catheter
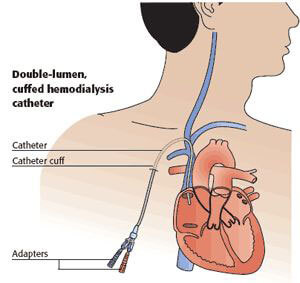 A dialysis catheter is like a giant IV which is placed in one of the biggest veins in the body – usually the jugular vein in the neck. This IV is very long, and its tip is placed in the right atrium of the heart. In this way, dialysis nurses use one port of the catheter to pull blood out of the body, and another port to put blood back into the body.
A dialysis catheter is like a giant IV which is placed in one of the biggest veins in the body – usually the jugular vein in the neck. This IV is very long, and its tip is placed in the right atrium of the heart. In this way, dialysis nurses use one port of the catheter to pull blood out of the body, and another port to put blood back into the body.
Dialysis catheters work well, but they are prone to infection. They also can hurt the large veins in the body, causing narrowing over time. Therefore, these catheters are only used for short time periods, until a more suitable access is ready to be used.